In the Darfur region, where the violence has taken an ethnic dimension, between 70 to 80 percent of health facilities are no longer functioning due to the lack of critical supplies and medical staff. There is a widespread shortage of critical supplies such as vaccines, nutrition commodities, and HIV medications, as well as a poor disease surveillance system. At the same time, overcrowded and dire conditions in gathering sites and camps exacerbate the risk of disease outbreaks, while people with chronic conditions are struggling to access the care and medicines they need to survive.

Sudan 2023 © Ahmad Mahmoud/MSF
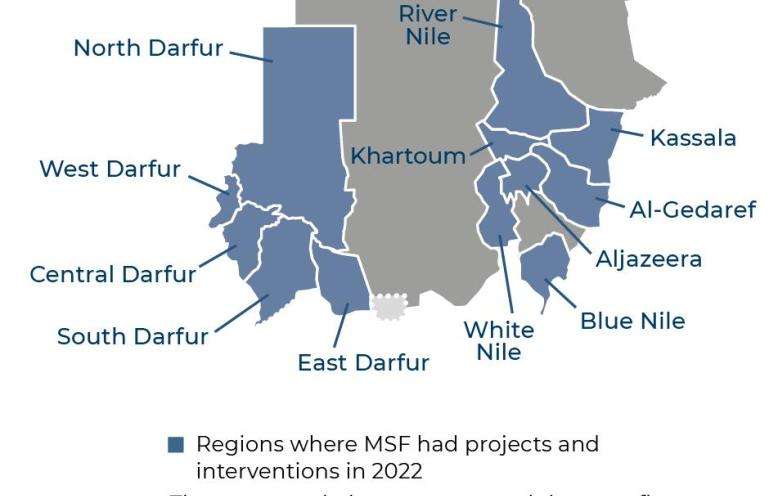
Sudan
In April 2023, intense fighting broke out across Sudan, including Khartoum and the Darfur region. MSF teams are providing medical care for people affected by this latest surge of conflict and other crises.
Overview
Sudan: Witnessing a life-and-death emergency on a massive scale
NEW YORK, April 10, 2024—The crisis in Sudan is a life-and-death emergency on a massive scale that has been overshadowed by other crises in the world, said Avril Benoît, executive director of Doctors Without Borders/Médecins Sans Frontières in the United States (MSF) USA, after visiting MSF teams in eastern Chad and in Sudan's Darfur region.
Read more
Our work in Sudan
Doctors Without Borders/Médecins Sans Frontières (MSF) continues to respond to multiple health issues during a turbulent year in Sudan, where the health care system is on the verge of collapse amid a devastating, ongoing conflict.

What's happening in Sudan?
For a year, large parts of Sudan have been experiencing ongoing violence, including intense urban warfare, gunfire, shelling, and airstrikes. The health system, already fragile before the conflict started, is struggling to cope with existing and emerging medical needs while facing overwhelming pressure from the destruction and looting of health facilities, acute shortages of utilities and medical supplies, and under-resourced health staff who are overworked without pay. As a result, people face significant challenges accessing medical care throughout the country. By the time many are able to access care, their condition has become critical.

How we're helping in Sudan
MSF teams in Sudan provide emergency treatment, surgical care, mobile clinics for displaced people, treatment for communicable and non-communicable diseases, maternal and pediatric health care, water and sanitation services, and donations of medicines and medical supplies to health care facilities. We also provide incentive pay, training, and logistical support to Ministry of Health staff who have gone overworked and underpaid for months, and we continue some of our medical activities that were in place before the start of the war.
How we're helping
586,800
Outpatient consultations
4,260
Children admitted to inpatient feeding programs
350
Tons of medical supplies delivered
1,950
Births assisted
230
Newborns admitted to hospitals
*Data from MSF International Activity Report 2022
More news and stories
Learn about MSF’s journalistic roots and our commitment to bear witness and speak out about the plight of the people we treat.



Learn about MSF’s journalistic roots and our commitment to bear witness and speak out about the plight of the people we treat.
How you can help
Not everyone can treat patients in the field. But everyone can do something.
Some humanitarian crises make the headlines—others don’t. Unrestricted support from our donors allows us to mobilize quickly and efficiently to provide lifesaving medical care to the people who need it most, whether those needs are in the spotlight or not. And your donation is 100 percent tax-deductible.



