
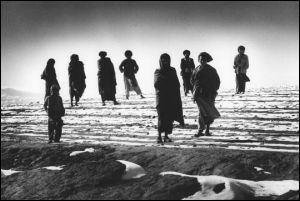
Sar-i Pul camp, Afghanistan, December 2001, where MSF has assisted displaced Afghans through a medical clinic and feeding center, and by providing drinking water. The number of Afghans forced to leave their homes because of lack of food continues to grow. © Tim Dirven/MSF |
The advent of the "war on terrorism" has generated a perception among some that the world changed fundamentally on September 11th 2001. But, for MSF and humanitarian action, the biggest challenge this new conflict has presented is an old, all too familiar one – that of remaining independent from political concerns to assure that civilians in need receive humanitarian help regardless of any other will. Political manipulation of humanitarian aid – from all sides – is as relevant in this "war against terror" as the wars we are more familiar with in Sudan, Angola and elsewhere.
Humanitarian action is a response to suffering, based on need alone, but the effective delivery of humanitarian aid is often obstructed for political and economic reasons. Over the last year MSF has been struggling to defend the independence of humanitarian aid, to ensure that the requirements of survival and dignity take priority.
In April 2002, MSF criticised the warring parties in Sudan for the appalling numbers of civilian deaths from disease and violence in the Western Upper Nile region. During 14 years' experience in the country we had been witness to how all parties to the conflict use violence against civilians – including rape, murder and assault – while denying them access to humanitarian aid. Six months later, MSF extended operations in southern Sudan to fight a deadly outbreak of kala azar (visceral leishmaniasis) that was threatening thousands of lives. The people there are exhausted by decades of war and extremely vulnerable to this disease due to insecurity, malnutrition and poor access to health care.
In Afghanistan, the principle of humanitarian aid was used by Western governments to gain support for military action. MSF teams that had been providing humanitarian aid in Afghanistan since 1979 were forced to leave Taliban-held areas for several months after September 11th 2001 due to increased insecurity (although our local staff members were able to keep programs running in many parts of the country). The US-led coalition began bombing a month after our expulsion, dropping food together with bombs as part of a "military-humanitarian" response. But this was to win favor in the West and to blunt resentment in Afghanistan, not to address the needs of the starving people. MSF denounced this act as damaging to the work of humanitarian aid agencies by confusing military and humanitarian objectives. Food aid must be appropriate and targeted to reach the most vulnerable, not scattered from the sky indiscriminately. A year later, though the needs are still huge, food is scarce and insecurity prevents the delivery of aid to many parts of the country, while international help falls far short of the promises.
International humanitarian law was created to protect and assist non-combatants in times of war and crisis. Yet, despite being invoked rhetorically by all sides, respect for its basic provisions is under threat. The political logic of today's "war on terrorism" seems to imply that because the "terrorists" do not, by definition, respect international conventions, anti-terrorist operations may therefore have a freer hand. The struggle to uphold humanitarian law suffers as a result, with disastrous consequences for the protection and assistance of civilian populations.
In the name of fighting terrorism, violations of international humanitarian law are increasingly being condoned. The limited attempts to restrain Israel's operations, which closed off the Jenin refugee camp for two weeks in April 2002, were rebuffed by the mantra "this is an anti-terrorist operation."
The global fight against terrorism has muted any international criticism of the abusive military operations conducted by Russian forces in Chechnya – a place of "total war" where any sense of responsibility to the citizens has been entirely obliterated by both sides, leaving no room for humanitarian aid.

Chipindo feeding center, Angola, May 2002. Chipindo was isolated first because of the war and then because of heavy rains. Between November 2001 and March 2002, famine and disease caused the death of some 4,000 children under the age of six in this area. © Sebastião Salgado/Amazonas Images
|
This particular concern was further demonstrated with the kidnapping of Arjan Erkel, MSF's head of operations in Dagestan, on August 12th 2002. By year-end, we had still heard no news. We have repeatedly urged the Russian authorities to maximize their efforts to solve the case and to secure Arjan's safe release. Kidnappings of staff of nongovernmental organizations around the same time demonstrate the risks civilians and relief workers run in this conflict-ridden region.
The heightened vulnerability of people in many of the places where MSF works was further highlighted by a United Nations High Commissioner for Refugees report at the beginning of the year detailing the problem of sexual exploitation, including violence, by aid staff of refugees in West Africa. Even though the claims made could not be substantiated, the issue is an extremely important concern for MSF, as it shows that refugees continue to be exposed to violence and exploitation. Our operational teams have been reviewing all training and disciplinary policies. But efforts to protect refugees from exposure to sexual violence and exploitation must go far beyond such actions and consider the increasing political disregard for refugee rights, and the erosion of the protection mandate.
The nutritional crisis in Angola this year is one of the clearest examples of why using aid to help a political cause hurts those in need of that aid. The country's 27-year civil war, in which civilians were targeted and abused by both sides, finally ended with a ceasefire in April 2002, and regions that had been cut off from humanitarian aid for over three years became accessible, revealing tens of thousands of starving people. We began one of our largest emergency relief operations ever, with 190 international volunteers and 2,000 national staff working around the clock in scores of feeding centers to try to save as many lives as possible.
But, despite high mortality and malnutrition rates, the aid effort was insufficient. While the responsibility for protecting and meeting the needs of the Angolan people lies first and foremost with the Angolan government, blame does not escape the international organizations, all of which were slow to respond in the first months of the crisis. Operations of many aid organizations were hindered by lengthy coordination with the United Nations, which was negotiating terms with the Angolan government with one overriding concern: maintaining the new peace. Meanwhile, thousands of people were dying of hunger. Humanitarian action became subservient to political calculations.
International news coverage of Angola, one of the worst food crises in the new millennium, was scant, and recent appeals for aid for that and other neglected crises such as Sudan or West Africa have been woefully under-funded. Clearly, the focus and priorities are elsewhere. The level of political commitment to global deprivation remains crassly insufficient, particularly in comparison with the push towards heightened military engagement and spending. The September 11th attacks immediately mobilized billions of dollars, as well as political, governmental and military resources, and public opinion. Meanwhile, resources to help the 14 million or so people who die yearly of infectious diseases are lamentably absent. Where is the coalition against infectious diseases? When will there be a massive push for a convincing solution to malaria, the number-one killer of children in Africa?
Effective new medicines to treat neglected diseases such as sleeping sickness, leishmaniasis and Chagas are lacking. These diseases primarily affect the poor and are ignored by both the public and private sector: from a purely profitdriven perspective, it is not an "attractive investment" to develop drugs for diseases affecting people without financial resources, and no public sector is presently filling that gap. To stimulate a response to the increasing need for effective medicines to treat such neglected diseases, MSF is working with partners to establish a Drugs for Neglected Diseases initiative (DNDi), a not-for-profit drug development capacity in the public sector. MSF's aim in initiating DNDi is to push for change in the way medicines are developed – according to health needs, not profit prospects – and urge governments to take up their responsibilities to ensure that effective medicines are available to all.
More must also be done to make sure that existing medicines are used effectively and are accessible to all who need them. The funds, the resources and the political will worldwide are all still inadequate. Almost 6 million people who are ill with AIDS today are still not receiving the life-prolonging medicines they need. They will die in the next few years, while tens of millions infected with the virus will soon share their fate. Our HIV/AIDS programs have expanded significantly over the last year. We now treat people with antiretroviral drugs in 11 countries and will continue to increase the numbers of our AIDS care programs. Over 2,000 patients currently benefit from antiretroviral treatment through our programs, with thousands more planned to benefit in the coming year. Clearly, our medical programs still only reach a fraction of those who need treatment, but our advocacy efforts help ensure that these limited programs serve as a provocation for those who are capable of and responsible for responding to the pandemic on a much larger scale. Our experience adds to the evidence that treating AIDS in resource-poor settings – once considered unviable – is possible even in remote rural areas. We are committed to expanding antiretroviral treatment in our projects, and will continue to advocate for access to treatment as a central part of AIDS prevention and care programs.
Furthermore, we cannot accept that millions of people continue to die of curable diseases like tuberculosis and malaria. In spite of many promises and proclamations, our medical teams on the ground have seen no change in the current situation. Global political engagement in the fight against infectious diseases still amounts to little more than indifference.
The humanitarian imperative requires responding to this shocking range of suffering according to needs, and meeting those needs adequately and effectively. In many places around the world, MSF is only able to meet the medical needs of marginalized, persecuted people because of our independence from political powers. We are able to do this thanks to the millions of individuals who support us worldwide and who, in doing so, have made the choice to support these principles. We will continue vigorously to protect the principle of independent humanitarian aid. At the same time, we call on all governments to exercise their fundamental responsibilities to protect the health, well-being and basic freedoms of their own citizens. The temporary nature of humanitarian work means that MSF intervention can never be part of the permanent solution. But our work can act as a reminder and a rebuke for those who are responsible for finding lasting solutions.
Dr. Morten Rostrup,
President, MSF International
Council
Rafael Vilasanjuan, MSF Secretary General


News Jul 26, 2024
ViiV must urgently help get more people on lifesaving HIV prevention m...
Read More
